Note how the newer versions of the UTL start to show inactivated concepts in the release. Since the UTL is based on SNOMED CT, you will notice that lab tests added to it in one release might also be inactivated in later releases. This inactivation process allows for outdated lab test codes to be flagged as inappropriate for current use. In the above graph, we plotted the now just the `new` concepts added in very release but also the number of concept inactivations where appropriate. Some of these inactivations are the result of feedback provided by the wider community about the appropriateness of the test.
Termlex worked closely with #NHSDigital and lead on the creating editorial principles and content of the UTL until 0.6.0. We continue to review and provide feedback on the UTL since then.

Read more about our work with NHS Digital on UTL content development and FHIR specification at Unified Test List, FHIR & UCUM: Pathology and Laboratory Medicine Standards.

Now we know that the UTL has both lab requests and results. But what exactly does it have in terms of content, coverage of disciplines, etc – inadvertent comparisions will be drawn to LOINC, NPU etc. While the UTL initially started with a focus on blood sciences, you can see a shift in the coverage of content.
For example in the graph below, note how the `microbiology` content grows between versions 0.6.0 and the latest 0.9.0 reflecting the broader roadmap of the standard development that the #NHSDigital team are pursuing.
Note: In order to declutter this graph for visualisation we deliberately omitted categories that represent less than 1% of the content. So the UTL as published has a lot more categories.
Within the context of the UK, it is more likely that wonder what the relationship between the extant (but legacy) Pathology Bounded Code List (PBCL) and the Unified Test List is. The PBCL given its long and complicated history is a mix of things that are likely requests but are used as proxies for results. However, the UTL tries to cleanly distinguish what are lab results (resultables) from lab requests (requestables). In fact, this is a distinction that is reflected in the UTL not just by publishing different files, but rather:
The PBCL's content was migrated from the Procedure hierarchy to the Observables hierarchy – but along the way it lost its modelling in SNOMED CT (or never had any). This explains why when you look at PBCL codes/names it is difficult at times to understand if is lab requestable or a resultable.
Here are some examples:
Within the UTL, these would clearly modelled as resultables:
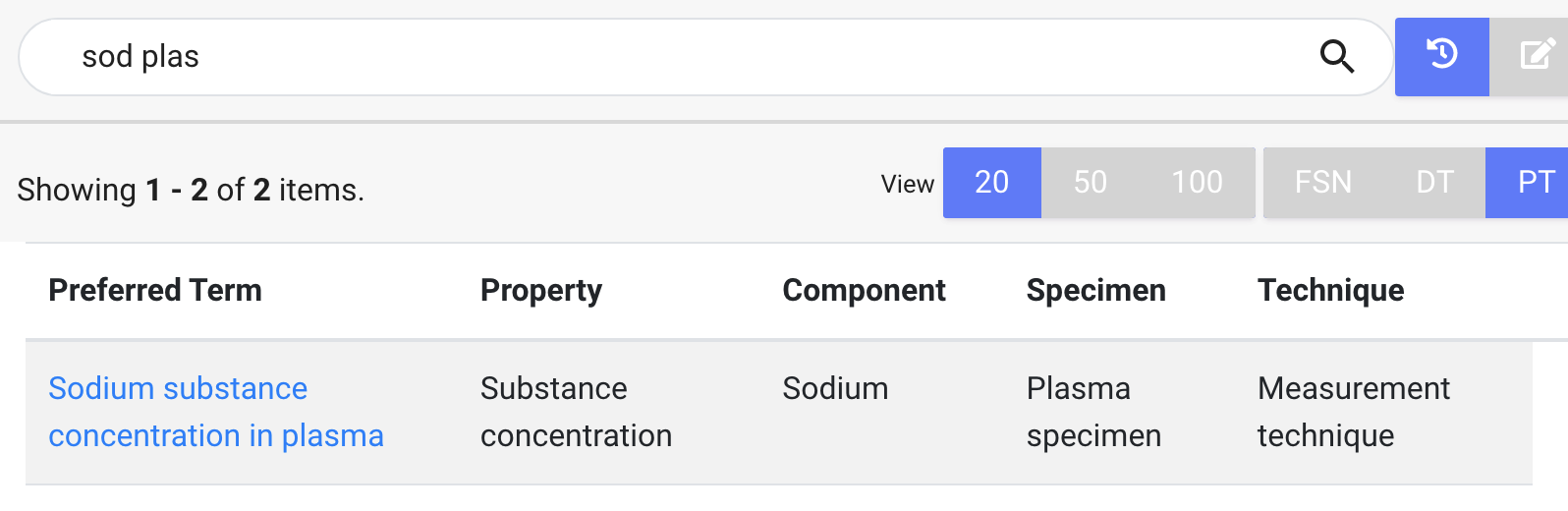
The good thing though is that UTL comes with definitions of these test results, which means we know Sodium substance concentration in plasma is actually described in terms of its `component`, `specimen`, `property` etc. All these would be missing from the corresponding equivalents in the PBCL.
However, you now have other options too in the UTL, if you wanted to be more specific where you are measuring the sodium in:
Pathnexus, our lab data harmonisation platform makes it very straight to evaluate all these possible options and to migrate your content to the UTL.
Want to migrate your existing data from the PBCL to the UTL, or want to use UTL, SNOMED CT or LOINC in your LIMS ?